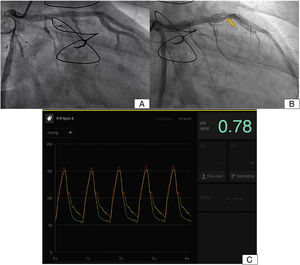
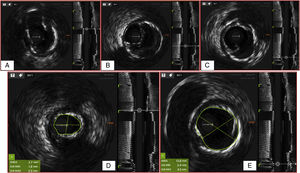

We present the case of a man who, 7 years earlier, had undergone a heart transplant for nonischemic dilated cardiomyopathy with well-managed immunosuppression and no signs of rejection. A follow-up coronary angiogram was performed at 1 year (figure 1A). The patient was admitted for progressive dyspnea, which now occurred even on minimal exertion. A coronary angiogram showed a pseudoaneurysm in the anterior descending artery and significant stenosis (figure 1B, arrow). Intracoronary ultrasound (video 1 of the supplementary data) showed a pseudoaneurysm with an entry point due to disruption of the intimal and medial layers of the arterial wall. There was significant stenosis (figure 2A-E) and the pressure wire assessment was positive for myocardial ischemia (instantaneous wave-free ratio, 0.78) (figure 1C).


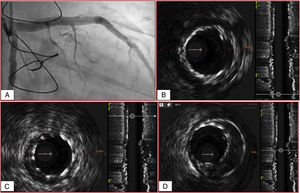
Intravascular ultrasound- and angiography-guided percutaneous coronary intervention with a drug-eluting stent was performed (secondary stent graft placement was planned in case the drug-eluted stent did not adequately seal the origin of the pseudoaneurysm). The communication observed between the arterial lumen and the adventitia prior to stent placement was successfully sealed (figure 3A-D and video 2 of the supplementary data).

Cardiac pseudoaneurysms are very rare. They are typically caused by blunt chest trauma, cardiac tumors, or iatrogenic injury during percutaneous coronary intervention. There have also been reports of spontaneous cases. Intravascular ultrasound is crucial for distinguishing pseudoaneurysms from true aneurysms (which involve all 3 layers). Pseudoaneurysms are saccular defects with a thin wall and a narrow neck. They do not contain the normal components of the artery wall and communicate with the arterial lumen though the breach in the wall.
Spontaneous coronary pseudoaneurysms in transplant recipient are extremely rare. We found no such cases in the literature.
FUNDINGNone
ETHICAL CONSIDERATIONSThe patient agreed to the publication of this report. Sex and gender were taken into account in the writing of this report.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCEArtificial intelligence was not used for this work.
AUTHORS’ CONTRIBUTIONSAll the authors contributed to reviewing the literature and drafting and revising the final version of this manuscript.
CONFLICTS OF INTERESTNone.