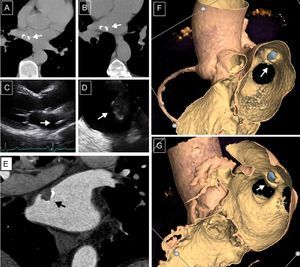
A 64-year-old male, with no past medical history, was sent to thoracic computed tomography to complete the study of several episodes of pneumonia within the last few years. A calcified annular lesion was incidentally found in the left atrium (Figures A and B), confirmed by transthoracic and transesophageal echocardiograms (Figures C and D), localized next to right superior pulmonary vein drainage. Because we suspected cardiac myxoma and considered surgical treatment as of choice in this sort of tumor, the mass was entirely removed and the diagnosis was confirmed by pathological examination. A contrast cardiac computed tomography was first ordered to exclude coronary artery disease and endoluminal views were attached (Figures E-G).

The lesion presented as a single heterogeneous mass, mobile and round, consistent with cardiac myxoma, with calcified foci (grey areas in Figures F and G). Dimensions 14 x 10mm. As clearly seen in the endoluminal images, the location was atypical, beside the pulmonary vein rather than the interatrial septum, as is more common. The differential diagnosis included other benign tumors such as lipomas (homogeneous masses), and fibroelastomas (which are frequent on cardiac valves and not seen on computed tomography if they are < 1.5cm). Although metastases are more prevalent than primary tumors, they usually affect the epicardium with metastases in other organs. Intracardiac thrombi are normally smaller, homogeneous, and immobile.
For these reasons, cardiac computed tomography performed in these patients to exclude coronary artery disease should include endoluminal reconstructions to enhance surgical results. These reconstructions have high accuracy in characterizing the morphology and location of myxomas, with no additional tests.