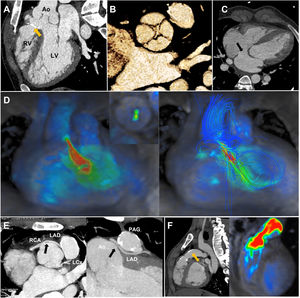

A 22-year-old man with a history of type I truncus arteriosus underwent surgery in the first year of life with implantation of a Contegra conduit (Medtronic Inc, United States) and closure of a ventricular septal defect (figure 1A). The patient underwent a reintervention at age 5 years with implantation of a pulmonary artery graft valved conduit (PAG). He had a truncal quadricuspid valve (figure 1B) and a wide ostium secundum atrial septal defect without significant dilation of the right ventricle (RV) due to coexisting PAG stenosis (figure 1C).

Echocardiography and cardiac magnetic resonance (CMR) were performed periodically. Four-dimensional flow CMR documented severe truncal valve regurgitation, with a 50% regurgitant fraction (figure 1D-left; video 1 of the supplementary data), streamline direction, and maximum flow velocity (figure 1D-right).
The anatomical orifice measured by cardiac computed tomography (CT) (Somatom Definition Flash 128-slice Siemens, Germany) was 0.53 cm2 Due to incomplete coronary visualization, a coronary CT was performed, revealing a common origin of the right coronary artery (RCA) and the left anterior descending artery (LAD) of the right-anterior sinus (figure 1E-left). The LAD had an interarterial course between the aorta (Ao) and the PAG (figure 1E-right). The left circumflex artery (LCx) emerged from the left-posterior sinus with normal course. Finally, PAG calcification was observed (figure 1F-left) with moderate stenosis (maximum systolic velocity 3 m/s quantified by 4-dimensional flow-CMR [figure 1F-right; video 2 of the supplementary data]) without current treatment indication. Replacement of the truncal valve, coronary artery bypass graft and ostium secundum atrial septal defect closure was considered. Advanced multimodal imaging aided the selection of the optimal time for surgery and planning of the most appropriate surgical technique. The authors confirm that written consent has been obtained from the patient for the publication of this article.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSAll authors contributed to data acquisition, conceptualization, writing, and revising the final version of the manuscript. The authors accept the responsibility defined by the International Committee of Medical Journal Editors.
CONFLICTS OF INTERESTNone.
Supplementary data associated with this article can be found in the online version, at https://doi.org/10.1016/j.rec.2023.04.006