ISSN: 0300-8932
Factor de impacto 2024
4,9
SEC 2012 - El Congreso de las Enfermedades Cardiovasculares

Sevilla,
18 - 20 de Octubre de 2012
4046. Ablación, síncope y fibrilación auricular
Fecha
: 20-10-2012 00:00:00
Tipo
: Comunicaciones mini orales
Sala
: Sala D (Planta 1)
4046-12. Hybrid percutaneous endocardial and thoracoscopic epicardial radiofrequency ablation of long standing persistent atrial fibrillation: initial experience
Alberto Carlos Weber Varela, Jürg Fuhrer, Thierry Carrel, Bernhard Meier y Hildegard Tanner del Schweizerisches Herzzentrum, Inselspital, Bern.
Background and objectives: To overcome the shortcomings of percutaneous catheter ablation and of minimal invasive surgical ablation, the hybrid ablation procedure has recently been introduced in order to combine the advantages of both techniques in the treatment of long standing persistent atrial fibrillation (AF). Our objective was to evaluate feasibility, safety and efficacy of this technique in our first cases.
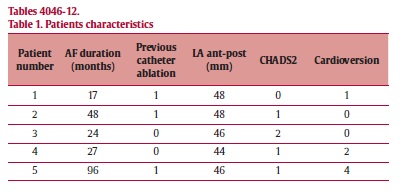
Methods: Between May 2010 and December 2011, 5 male patients with long standing persistent AF, mean age 50.8 years (range 42-62 years), underwent a single step hybrid minimally invasive surgical treatment of persistent AF combined with a percutaneous endocardial ablation. Both techniques employed radiofrequency energy during general anesthesia in the EP lab. Preoperative patient characteristics are depicted in table 1. The surgical procedure is a closed-chest video assisted right monolateral thoracoscopic epicardial ablation encircling all pulmonary veins in a box lesion. Two ablation sequences were carried out at target temperatures of 65 and 75 °C, 120 sec per each ablation; the power is adjusted according to the target temperature (max 150W). In addition, percutaneous catheter assessment of pulmonary vein isolation and additional lesions if necessary were performed. Rhythm follow-up using 7-day ECG recording was performed at 3,6 and 12 months.
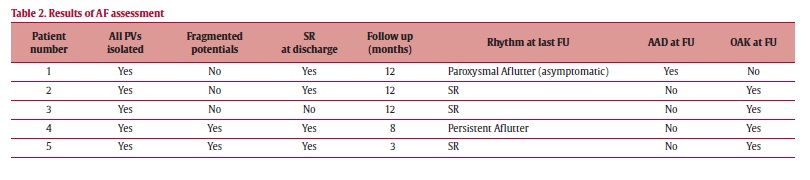
Results: There were no intraprocedural complications. All patients were extubated in the EP lab. Median procedure time was 240 min (range 120-395 min). Median total X-Ray time was 19.4 (range 11.4-59.6 min). No patient required intensive care or blood tranfusion. One patient presented a transient diaphragmatic paresis and one patient suffered a post-interventional transient bradycardia. Mean in-hospital length of stay was 6 days. Results of AF assessment are depicted in table 2.
Conclusions: The single step hybrid surgical-epicardial and percutaneous-endocardial ablation treatment of long persistent AF is feasible and seems to be safe in an initial small series. Optimal interdisciplinary collaboration between electrophysiologists, cardiac surgeons and anesthesiologists is crucial. The efficacy of this treatment must be further studied in larger series and longer follow up.
Comunicaciones disponibles de "Ablación, síncope y fibrilación auricular"
- 4046-1. Presentación
- Juan M. Cinca Cuscullola, Barcelona y Concepción Moro Serrano, Madrid.
- 4046-2. Resultados a largo plazo tras la estratificación del riesgo en pacientes con Síndrome de Brugada en una comunidad autónoma
- Juan Pablo Flórez Muñoz, David Calvo Cuervo, José Manuel Rubín López, Beatriz Samaniego Lampón, Diego León Durán, José Julián Rodríguez Reguero, Cesar Morís de la Tassa y José Luis Lambert Rodríguez del Hospital Universitario Central de Asturias, Oviedo (Asturias) y Hospital de Cabueñes, Gijón (Asturias).
- 4046-3. La caracterización de la cicatriz miocárdica predice a largo plazo la terapia de resincronización cardiaca
- Reinder Evertz, Antonio Berruezo Sánchez, Franco Merschón, Juan Fernández-Armenta Pastor, David Andreu Caballero, José María Tolosana Viu, Lluís Mont Girbau y Josep Brugada Terradellas de la Sección de Arritmias, Servicio de Cardiología, ICT, Hospital Clínic, Universitat de Barcelona, Barcelona.
- 4046-4. Remodelado de venas pulmonares tras la ablación de fibrilación auricular: resultados de un estudio comparativo entre crioenergía y radiofrecuencia
- Nicasio Pérez Castellano, Susana Martín Garre, Asunción Conde López-Gómez, Victoria Cañadas Godoy, José M. Aguirre, Pilar Cabrerizo Sanz, Julián Pérez-Villacastín y Carlos Macaya Miguel del Hospital Clínico San Carlos, Madrid.
- 4046-5. El análisis con cámara termográfica de las lesiones de radiofrecuencia producidas por cuatro catéteres irrigados abiertos revela diferentes perfiles de calentamiento del tejido
- Roberto Molina-Morúa, María José Ángulo Hernández, María Jesús García Torrent, Jorge G. Quintanilla, Carolina Curiel Llamazares, Javier Moreno, Carlos Macaya y Julián Pérez-Villacastín del Hospital Clínico San Carlos, Madrid y Universidad Rey Juan Carlos, Madrid.
- 4046-6. Relación de los ítems empleados en las escalas de riesgo de síncope con recurrencia, mortalidad y reingreso hospitalario
- Juan Parejo Matos, Eva María Cantero Pérez, Álvaro Arce León, Agustín Fernández Cisnal, Mariano Zamora Sierra, Nieves Romero Rodríguez y Gonzalo Barón-Esquivias del Área del Corazón del Hospital Universitario Virgen del Rocío, Sevilla.
- 4046-7. Prevalencia de fibrilación auricular paroxística asintomática en la monitorización continua con Holter subcutáneo en pacientes con accidente cerebrovascular isquémico criptogénico
- María de Gracia Sandín Fuentes, Fernando Malpica Cervantes, Jerónimo Rubio Sanz, Emilio García Moran, Juan Manuel Villadeamigo Romero, Esther Rojo, J.F. Arenillas y Alberto San Román Calvar del ICICOR, Hospital Clínico Universitario, Valladolid y Servicio de Neurología, Hospital Clínico Universitario, Valladolid.
- 4046-8. Ablación de taquiarritmias supraventriculares después de cirugía cardiaca. Características y seguimiento a largo plazo
- Ignasi Anguera Camós, Miguel Álvarez, Javier Jiménez-Candil, Mari Fe Arcocha, Javier García Seara, Aurelio Quesada, Antonio Hernández Madrid y Rafael Peinado del Hospital de Bellvitge, L'Hospitalet de Llobregat (Barcelona).
- 4046-9. Eficacia del aislamiento de una vena pulmonar o de un tronco venoso pulmonar único "culpable" en la ablación de la fibrilación auricular paroxística
- Eficacia del aislamiento de una vena pulmonar o de un tronco venoso pulmonar único "culpable" en la ablación de la fibrilación auricular paroxística
- 4046-10. Entropía para analizar la recurrencia de la fibrilación auricular en los procedimientos de ablación
- Raquel Cervigón Abad, Javier Moreno Planas, Francisco Castells Ramón, José Millet Roig, Jorge García Quintanilla, Nicasio Pérez Castellano y Julián Pérez-Villacastín de la Escuela Politécnica de Cuenca, Cuenca, Hospital Universitario Clínico San Carlos, Madrid y Universidad Politécnica, Valencia.
- 4046-11. El análisis de los parámetros de impedancia en ablación a alta potencia no predice la ocurrencia de POPS en un modelo experimental en muslo de cerdo perfundido
- Carolina Curiel Llamazares, Jorge G. Quintanilla, Roberto Molina-Morúa, Javier Moreno, María Jesús García-Torrent, Pablo González, Carlos Macaya y Julián Pérez-Villacastín del Hospital Clínico San Carlos, Madrid.
- 4046-12. Hybrid percutaneous endocardial and thoracoscopic epicardial radiofrequency ablation of long standing persistent atrial fibrillation: initial experience
- Alberto Carlos Weber Varela, Jürg Fuhrer, Thierry Carrel, Bernhard Meier y Hildegard Tanner del Schweizerisches Herzzentrum, Inselspital, Bern.
Más comunicaciones de los autores
- Carrel, Thierry
- Fuhrer, Jürg
- Meier, Bernhard
- Tanner, Hildegard
- Weber Varela, Alberto Carlos